The question stem is describing a mitochondrial disease, which commonly present with lactic acidosis. There is an increase in anaerobic forms of energy production (glycolysis). The mitochondria are faulty, so they can’t use the end product of glycolysis (pyruvate) in TCA. Instead pyruvate is shunted over and is used by LDH (lactate dehydrogenase) to generate pyruvate.
Aside: Recall that LDH uses NADH and generates NAD+. Deficiency of LDH can lead to loss of regeneration of NAD+ and inhibits glycolysis.
This is representative of leukoplakia, a pre-cancerous lesion of squamous cells. In order for it to spread to distant sites, it must first invade through the basement membrane/submucosa. Could be confused with oral hairy leukoplakia (which also is a white patch that classically arises on the lateral tongue). However, oral hairy leukoplakia is not pre-cancerous and is often associated with EBV infections or people that are severely immunocompromised.
Seeing fat in the stool would clue you in to whether or not the treatment regimen is working. Supplementing with pancreatic enzymes means that you should NOT see for fat in the stool.
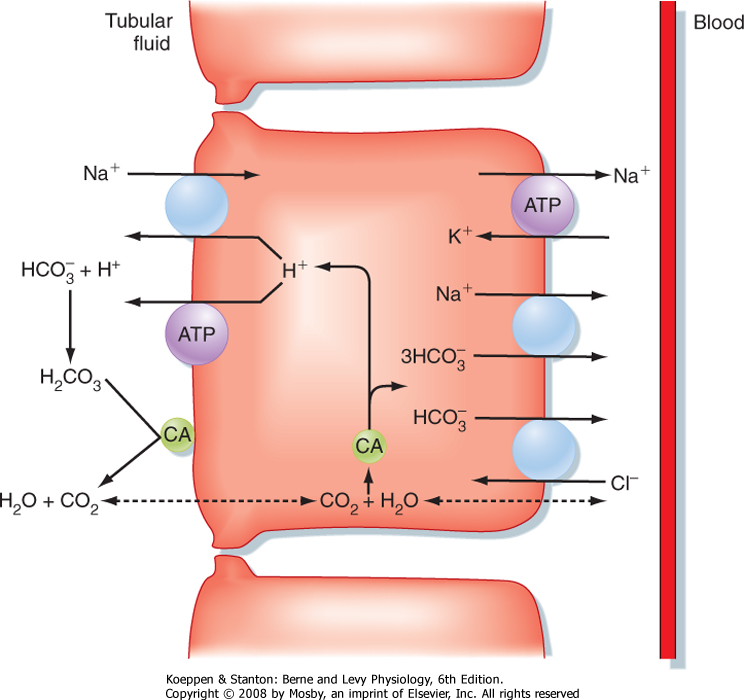
Since you're losing all your bicarb into your pee, you would expect the pH to be more alkaline. Also, since there is decreased Na+/H+ antiport, there is less sodium reabsorbed and therefore increased loss of free fluid to the urine.
{kind=link}
{kind=link}
Could also use the patient's age to make the differential. Age is a risk factor related to breast cancer (common in post-menopausal women, unless there's a history of breast cancer in the family).
Fibrocystic changes and fibroadenomas are usually common in premenopausal women.
No discharge noted, so it's not an intraductal papilloma.